
Brief anatomy review before beginning: The cornea is the clear part of the front of your eye. It is made up of 5 layers (or maybe 6 given recent research that suggests another layer- “Dua’s layer”-exists between the stroma and Descemet’s membrane). The outer layer is the epithelium, the second layer is Bowman’s membrane, the third and largest layer is the stroma, beneath that is Descemet’s membrane, and last is the endothelium.
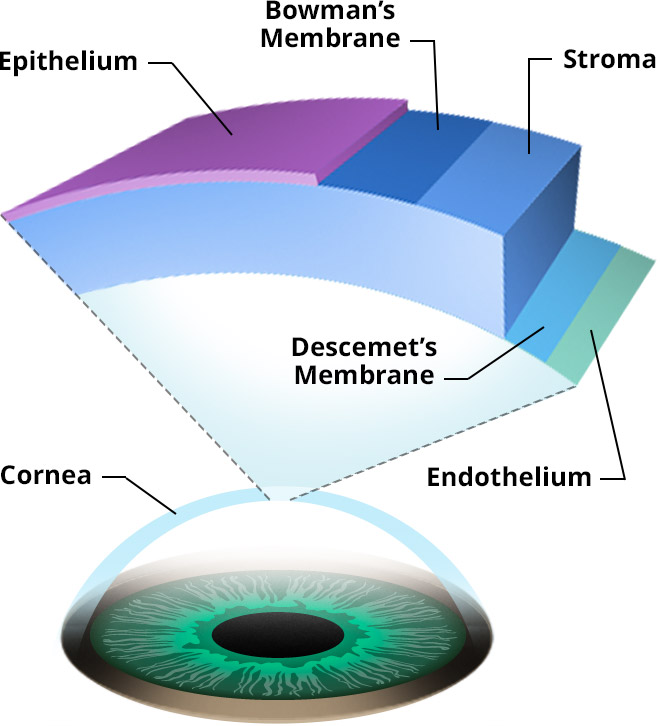 |
| The layers of the cornea Image: All About Vision |
What is Recurrent Corneal Erosion?
Recurrent corneal erosion syndrome, or RCE, is a condition in which the outer layer of the cornea (the epithelium) repeatedly sloughs off due to poor adhesion to the tissue beneath it. This poor adhesion is most often due to either past superficial trauma or an inherited condition that affects the outer layers of the cornea (ie: EBMD/map-dot-fingerprint corneal dystrophy, lattice corneal dystrophy, Reis-Bücklers corneal dystrophy, granular corneal dystrophy). Microerosions are smaller erosions with symptoms that last for a few minutes or hours, and they are more associated with corneal dystrophies. Macroerosions, on the other hand, are larger erosions with symptoms that last for many hours or even days, and tend to occur more in cases of past corneal trauma (1).
Why does it happen?
The basal layer of the epithelium is the innermost layer of the epithelium. It adheres to the underlying basement membrane via something called an adhesion complex. This complex is made up of hemidesmosomes and collagen fibrils- fancy words to say that it basically anchors the outer layers of the cornea. Due to trauma and/or dystrophy, the basement membrane is deposited abnormally, causing irregularities in the layers and disrupting the adhesion complexes. This weak adhesion leaves the epithelial cells more prone to sloughing off, or eroding.
A history of trauma is present in roughly half of RCE cases (2), especially when the trauma involved a fingernail or tree branch. Trauma disrupts the adhesions that exist in the epithelium. The subsequent inflammation from the injury also causes a breakdown in the adhesion complex. Matrix metalloproteinases (MMPs) are inflammatory mediators that are thought to play a role in degrading the protein and collagen matrix of the corneal tissue, leading to erosion. I picture MMPs as little ninjas that sneak in with swords to break apart the scaffolding proteins in the adhesion complex. People with RCE have been found to have increased MMP 2 and 9 levels in the tear film and epithelial cells (3,4).
Patients with EBMD, or other dystrophies affecting the outer layers of the cornea, experience similarly poor adhesion of the epithelium cells to the underlying basement membrane, due to changes in the cells of the epithelium and/or basement membrane.
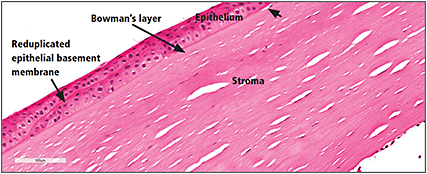 |
| A cell slide showing an irregular epithelial basement membrane Image: Ophthalmology Management |
What are the symptoms?
RCE presents with a painful, irritated, watery, red eye. Light sensitivity and blurry vision can result as well.
These symptoms are usually experienced during sleep or upon wakening. It tends to happen during sleep when your body enters REM sleep, because the eyes actually make small, quick movements from side to side (hence the name Rapid Eye Movement, aka REM). While you sleep, superficial corneal swelling and surface dryness occur, which can weaken the adhesion within the cornea and/or foster lid sticking. So when you open your eyes, the lids have a shearing effect, dislodging the epithelial cells and causing an erosion.
How is RCE treated?
The initial goal of treatment is to heal the cornea and relieve symptoms. The next goal is to prevent or minimize recurrence by creating new, stronger junctions within the cornea.
To keep things organized, we will break the treatment options up into two categories: medical and surgical treatments. Let’s begin by discussing some of the medical treatments for RCE:
- Lubrication. This is the first-line treatment for RCE. The goal here is to help heal the cornea and prevent the inside of the eyelid from sticking to the outside of the cornea while it’s healing.
- Artificial tear eyedrops. Preservative free artificial tears are best, and they are to be applied several times a day (every 1-2 hours) during acute episodes.
- Ointments. Hypertonic ointments (sodium chloride 5%) are good because they reduce swelling in the cornea while also lubricating the eye. Artificial tear ointments are also good options. For my RCE patients, I recommend applying artificial tear ointment before bedtime every night preventatively. Using an eye mask while sleeping has also helped some of my RCE patients avoid recurrences. Or you could wear a helmet to sleep, like this guy (that’s a joke- don’t do that).
- Punctal occlusion. This is an option if lubrication with drops and ointments doesn’t do the job. A punctal plug is essentially a cork that we place in the drainage system of the eye, to keep tears on the surface of the eye longer. Short term plugs are made of collagen and dissolve over time, and long term plugs are made of silicon.
- Bandage soft contact lenses (BSCL). Wearing a contact lens helps prevent lid/epithelial adhesion and the shearing effect we discussed earlier. The protection offered by the BSCL allows the adhesion complex to mature without disruption. The epithelium regenerates and symptoms subside within a few days (roughly 3-7 days), but the adhesion complex takes a few months to stabilize. Thus, treatment should be ongoing for at least 2-3 months (5). A study showed that after 3 months of treatment with a BSCL, 75% of the RCE patients were without recurrence after 1 year (6). It is important to note that a patient wearing a BSCL must visit their optometrist or ophthalmologist at regular intervals to replace the contact lens and to make sure there are no complications.
- Anti-MMP therapy. As discussed earlier, MMPs play a role in degrading the adhesion complex. A category of antibiotics called tetracylines have anti-MMP properties, as do steroids. Doxycycline is the tetracycline used most often in this case. A combination of both oral doxycycline and topical steroids has been shown to be effective in treating RCE and preventing recurrences. One study found that eight weeks after starting the combination treatment, 71% of patients were symptom free. At 6 months, 83% denied any symptoms suggestive of relapse and at 12 months, 73% were free and clear (7). A second study followed a similar method and found no recurrences amongst the test subjects over an average followup period of 21.9 months. When the researchers cultured the corneal epithelium in the test subjects, they found that this combination treatment produced a statistically significant decrease in the amount and activity of MMP-9 (8).
- Autologous serum. This is essentially an eyedrop made from a patient’s own blood serum. Sounds weird, I know. The patient has blood drawn, the blood is spun around to separate out all the different components (centrifuged), and the serum is removed, diluted, and bottled. The properties of blood serum are similar to those of tears, so this method is used to treat various ocular surface diseases. While this sounds great, it is not the cheapest or easiest treatment option out there. But it does appear to be effective. Over a followup range of 1-2 years, 85% of RCE patients treated with autologous serum for 6 months had complete healing with no recurrences (9).
For chronic cases and/or frequent recurrences, bigger guns may be needed. Here are a few surgical options available:
- Anterior stromal puncture (ASP). This is a procedure in which a tiny needle, or a Nd:YAG laser, is used to poke through the outer cornea to the beginning of the third layer of the cornea. The idea is that the puncture cause inflammation and creates pinpoint scars that strengthen the adherence of the epithelium to the underlying tissue. Since corneal scarring can affect vision, it is best to use this procedure if the area of erosion is NOT in the center of the cornea.
- Epithelial debridement and diamond bur polishing. This involves purposefully removing the weakly adhered epithelial cells and basically wiping the slate (basement membrane) clean. With the eye numbed, the loose epithelial cells are removed, leaving the outer edge of the cornea intact. Diamond bur polishing can be done after debridement and has been shown to reduce recurrence rate when compared to debridement alone (10). The bur basically buffs Bowman’s membrane to create a smoother surface. A bandage soft contact lens is used, as well as drops for lubrication, protection against infection, and pain relief as needed.
- Amniotic tissue membrane can be used here instead of a BSCL. Their role in RCE treatment would be similar to a BSCL, except that the amniotic membrane tissue has therapeutic qualities that help heal the cornea. Amniotic tissue is actually made up of some of the same collagens and proteins that the cornea is, and has anti-microbial and anti-inflammatory properties. Sutureless amniotic membranes can be cryopreserved (ProKera) or dehydrated (AmbioDisk or BioD Optyx). A study was done using ProKera following epithelial debridement; of the 11 eyes that were treated, only one eye had a recurrence over a followup span of 10-16 months (11).
- Phototherapeutic keratectomy (PTK). The first layer of the cornea is removed (similar to the method described above), and an excimer laser is used to remove a small amount of the second layer of the cornea (Bowman’s membrane), smoothing away irregularities. This allows formation of a new basement membrane and adhesion complex. Animal studies have shown an increase in anchoring proteins following excimer laser treatment (12). A BSCL or amniotic membrane is placed on the cornea while it heals. Like debridement, it takes a few days to recover; however it is more expensive since a laser is used and it is performed in an operating room. In a study of 76 eyes with RCE treated with PTK, only 11% had recurrences. Of those that had recurrences, only 25% continued to have recurrences after retreatment with PTK (13). Recurrence rates tend to be lower if corneal dystrophy is NOT the cause of RCE.
CliffsNotes: RCE is a condition in which the cells of the outer cornea repeatedly slough off. It is usually a result of past trauma or an inherited corneal condition. It hurts. A lot. But there are medical and surgical options that you and your optometrist or ophthalmologist can discuss to heal the erosion when it happens and to help prevent it from happening again.
Additional Recommended Resources: